
The Medical Affairs Onboarding Guide: What New Hires Need (And Managers Should Know)
By Laragh de Bhulbh, PhD MSc Pharm Med, MFPM (Hon) Founder, Wolf Medical Ltd

TL;DR
Medical Affairs is evolving into a strategic pillar of pharmaceutical companies, alongside R&D and Commercial. Yet a mismatch exists; most new hires are brought in for their clinical and scientific expertise and then expected to figure out the rest of the role by osmosis. This guide covers what Medical Affairs actually does across the product lifecycle, the critical promotional vs non-promotional distinction, the recurring questions new hires ask, and what closes the onboarding gap that the industry rarely names.
"You'll learn on the job"
If you're new to Medical Affairs, you've probably heard this. Possibly on day one. Possibly in the interview.
It's not said unkindly. It's how most of us learned. It's how our managers learned.
But here's the uncomfortable truth: "you'll learn on the job" isn't onboarding. It's the absence of onboarding wearing onboarding's name badge.
And in a function that McKinsey now describes as the strategic third pillar of pharma alongside R&D and Commercial, that absence has real consequences.
This guide is for people in their first two years in Medical Affairs - and the managers responsible for them. It covers what the role actually looks like, what it does across a product's lifecycle, the line between promotional and non-promotional activity, and the questions new hires ask quietly because they don't want to ask them out loud.
It's the article I wish someone had given me on day one.
What is the role of the Medical Affairs department in pharma?
Medical Affairs is the strategic function inside a pharmaceutical company that sits between the science and the people who use it.
That's the short version. The longer version matters.
In its 2030 vision, McKinsey identified Medical Affairs as the third pillar of pharmaceutical companies - coequal with R&D and Commercial / Market Access. Not a support function. A pillar. That language is not accidental. It signals where the industry is going, even where companies haven't restructured to reflect it yet.
What does that mean practically?
Medical Affairs is the function that:
→ Engages with healthcare professionals and patient organisations as a scientific peer, not as a sales channel
→ Translates external scientific insight back into the company, so strategy is shaped by what's actually happening in practice
→ Educates internal cross-functional partners - Marketing, Commercial, Market Access - on the data and the disease area
→ Generates and synthesises clinical evidence beyond the registration trials
→ Acts as the bridge between R&D and the market
That last one is the easiest way to remember it. Medical Affairs is the bridge.
R&D develops the science. Commercial sells the product within its licence. Medical Affairs translates between the two, gathers insight from outside, and ensures the company's understanding of the disease, the patient, and the evidence is constantly being refreshed.
The function operates differently from Commercial (i.e Marketing and Sales) in one fundamental way. Medical Affairs activities are strictly non-promotional. More on that below - it's important enough to deserve its own section.
The red thread: Medical Affairs across the product lifecycle
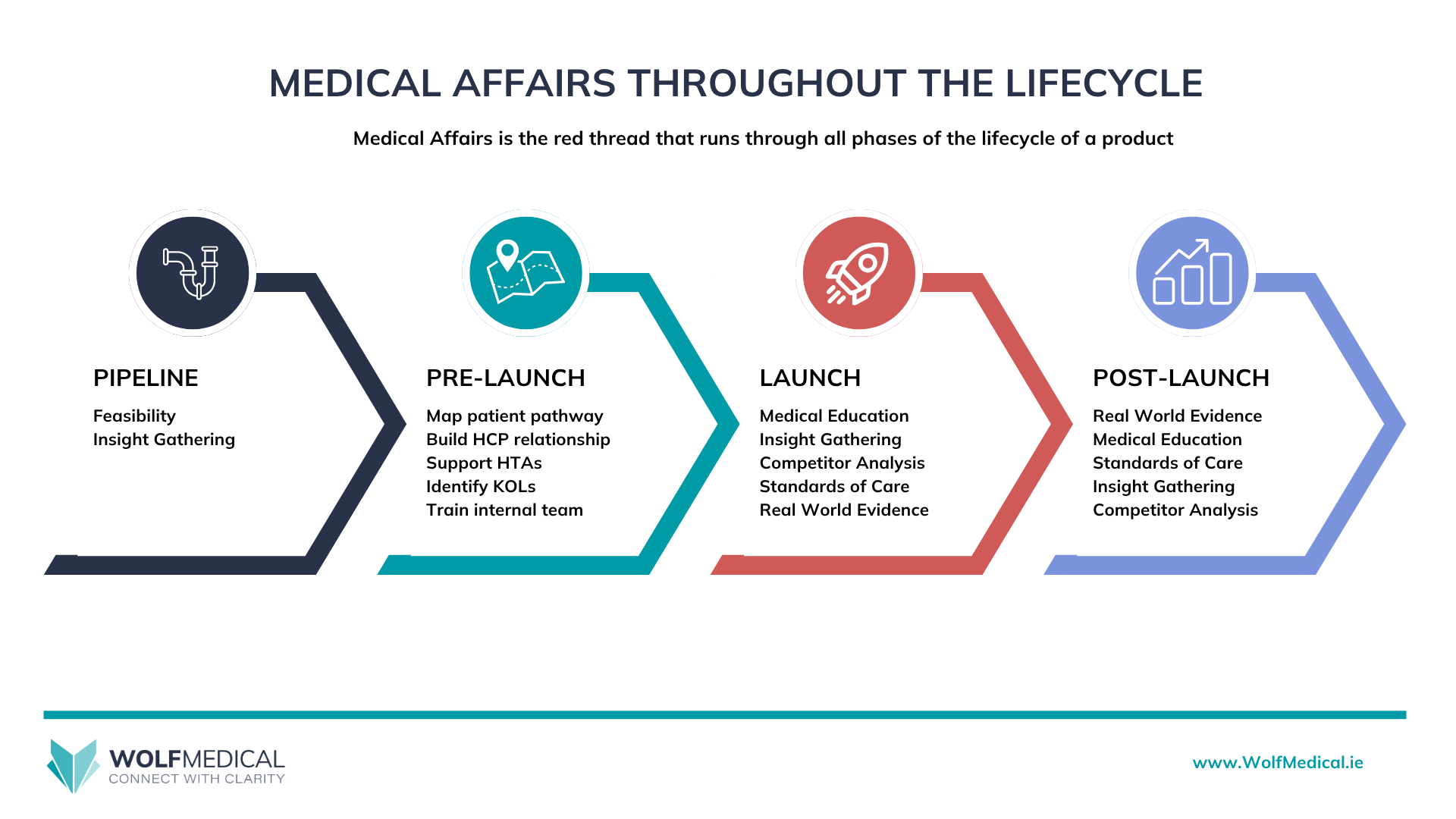
One of the most useful ways to understand Medical Affairs is to think of it as the red thread that runs through a medicine's entire lifecycle.
A medicine moves through phases. Pre-clinical. Phase I, II, III trials. Regulatory submission. Launch. In-market. Eventually, loss of exclusivity.
Commercial teams typically engage heavily from late pre-launch through early in-market. R&D engages heavily in development and tails off after launch. Medical Affairs engages across all of it. The activities change. The strategic role doesn't.
This is why the question "what does Medical Affairs do?" has no single answer. The answer depends on where the medicine is.
Medical Affairs lifecycle diagram
Pre-launch: laying the foundations
Years before a medicine reaches the market, Medical Affairs is already working.
In this phase, the function focuses on:
→ Mapping the patient journey - understanding how patients currently move through the healthcare system, where the diagnostic and treatment gaps are, and where the medicine could change that journey
→ Building relationships with Key Opinion Leaders (KOLs) - clinicians who shape practice in the therapy area, who will need to be familiar with the data well before launch
→ Conducting clinical feasibility work - supporting decisions about trial design, site selection, and protocol refinement
→ Gathering insight - through advisory boards, scientific exchange, and structured listening, building the company's understanding of unmet need and how the data will land
→ Supporting Health Technology Assessment (HTA) preparation - working with Market Access on the evidence base needed for reimbursement conversations
The work in this phase is foundational. Done well, it makes launch dramatically easier. Done badly - or skipped because the affiliate didn't assign headcount early enough - it costs the launch dearly.
Launch: establishing the narrative
When a medicine launches, the focus shifts.
Medical Affairs at launch is responsible for:
→ Establishing the clinical narrative - how the data is talked about, what it means in context, where the medicine fits in the treatment paradigm
→ Proactive medical education - symposia, scientific meetings, educational materials that help HCPs understand the disease and the data
→ Competitor analysis - staying close to what's happening elsewhere in the space and how that changes the conversation
→ Monitoring standards of care - understanding how the disease is diagnosed, monitored and treated, tracking how the medicine is being adopted, what's working, so that patient care continues to evolve
→ Supporting cross-functional alignment - making sure Marketing, Market Access, and Commercial are working from the same scientific foundation and that this translates into the field
Launch is the most visible Medical Affairs phase. It's also the phase where new hires most often join - and where the lack of foundational training shows most acutely.
Post-launch: sustaining the value
After launch, the function evolves again.
Post-launch Medical Affairs focuses on:
→ Real World Evidence (RWE) generation - building the body of evidence on how the medicine performs in real clinical practice, outside the controlled environment of registration trials
→ Late-phase studies and investigator-initiated research - supporting clinically meaningful questions the registration trials didn't answer
→ Continued KOL engagement - relationships don't end at launch; they deepen
→ Monitoring the competitive landscape - new entrants, new data, new guidelines, how your medicine compares, where your pipeline products fit in
→ Supporting line extensions and label updates - generating the evidence base for new indications, new populations, new formulations
The post-launch phase is where Medical Affairs proves its long-term strategic value. A medicine well-supported by Medical Affairs into in-market typically outperforms one where the function's effort tails off after launch.
The red thread holds the whole thing together. Same function, same strategic role, different specific activities depending on where the medicine is.
What's the difference between Medical Affairs and Commercial?
Medical Affairs and Commercial (Marketing and Sales) are both pharma functions that engage with healthcare professionals, but they operate under fundamentally different rules. Commercial is responsible for promoting the product to encourage prescribing -restricted to on-licence information and regulated by industry codes (ABPI, IPHA, EFPIA, Medicines Australia). Medical Affairs is responsible for scientific exchange - non-promotional, peer-to-peer, and able to discuss off-licence topics reactively when an HCP raises them. Commercial talks about the product; Medical talks about the disease area and the science. Both are needed. Both are legitimate. The line between them is one of the most important things a new Medical Affairs hire learns.
Promotional vs non-promotional: the line that defines Medical Affairs
This is the distinction new hires most often think they understand and most often don't.
In pharma, activities directed at HCPs fall broadly into two buckets.
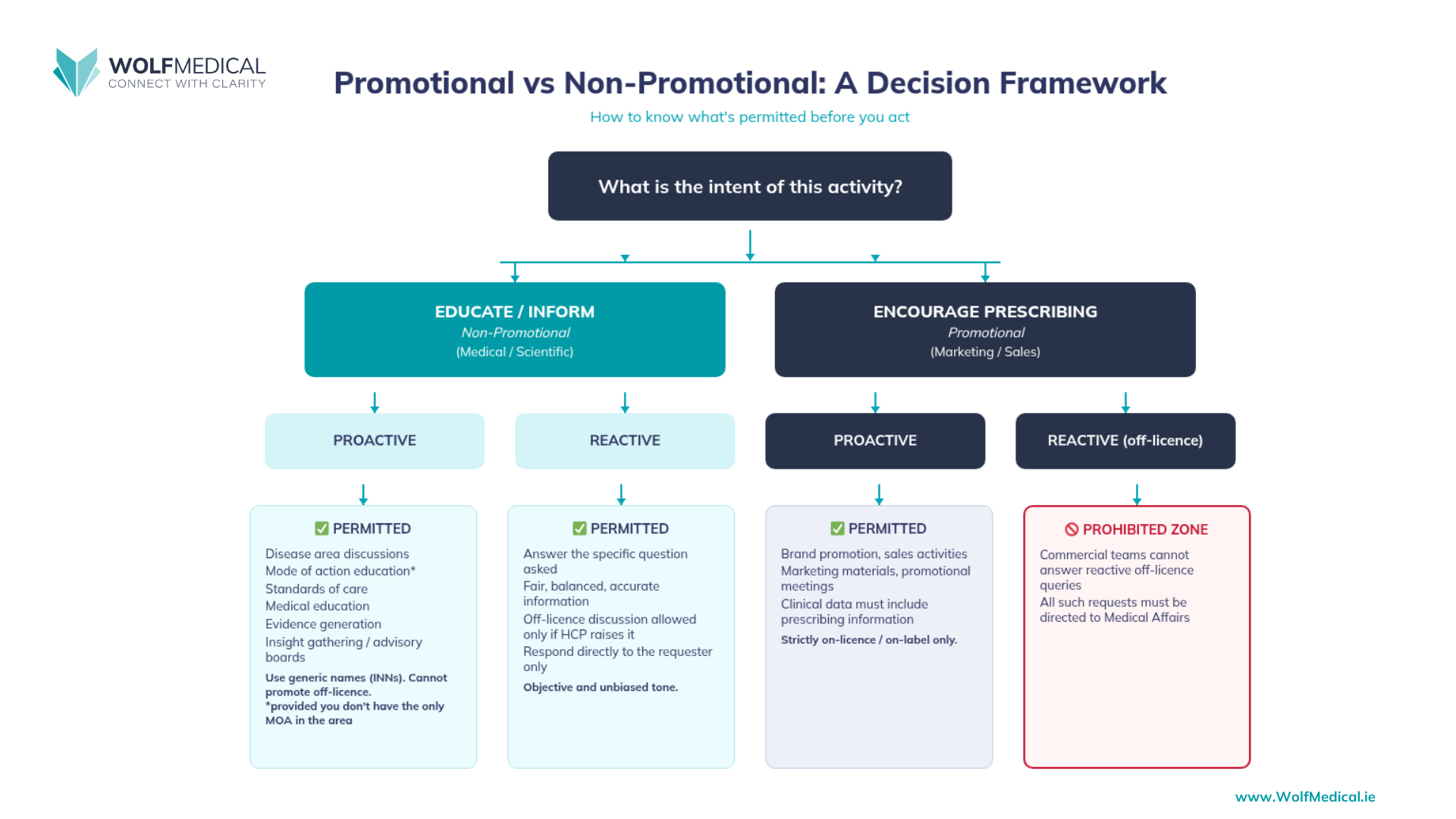
Promotional activities are intended to encourage and increase the prescribing or use of a medicine. They're owned by “Commercial” functions such as Marketing and Sales. They're restricted to information within the medicine's licence - its approved indications, dosages, populations, and methods of use. They're heavily regulated by industry codes (ABPI in the UK, IPHA in Ireland, EFPIA across Europe, and equivalents elsewhere).
Non-promotional activities are scientific in nature, not intended to drive prescribing, and operate under a different set of rules. It’s about improving the standard of care for patients. Medical Affairs activities are strictly non-promotional.
This isn't a soft distinction. It's a structural one.
What it means in practice:
→ Medical Affairs can engage in peer-to-peer scientific exchange with HCPs - sharing scientific perspectives, having genuine clinical conversations
→ Medical Affairs can have reactive discussions about off-licence topics - different dosages, different populations, different methods of administration - when an HCP raises them, providing fair, balanced, accurate information
→ Medical Affairs cannot proactively discuss or promote off-licence use, and cannot frame any activity in a way that's intended to influence prescribing
→ Advisory boards run by Medical Affairs are convened to gather insight, not to educate HCPs about a product
→ Medical education focuses on the disease area, the science, the standards of care - not the product as a commercial proposition
For new hires, the most useful mental model is this: Commercial talks about the product. Medical talks about the disease area and the science.
Both are needed. Both are legitimate. The line between them is one of the most important things a new Medical Affairs hire learns - and one of the things most often taught badly. The fear of overstepping often causes Medical Affairs to be overcautious, limiting the efficacy of the role.
Promotional vs Non-Promotional decision framework
10 Questions Every New Medical Affairs Hire Asks
Inside our Medical Affairs Essentials community and across the companies I work with the same questions surface week after week. Questions from bright, qualified, recently-hired people who are quietly worried they're the only one asking. They're not. If you have the question, guaranteed someone else does too.
Here are the ones that come up most. Brief, practical answers below each.
"What does Medical Affairs do at each stage of the product lifecycle?"
Different things at each phase. Pre-launch: patient journey mapping, KOL development, feasibility, insight gathering, HTA preparation. Launch: clinical narrative, medical education, competitor analysis, cross-functional alignment. Post-launch: RWE, late-phase studies, line extensions, sustained KOL engagement. Same function, different activities depending on phase. See the lifecycle section above.
"How do I get out in front of HCPs?"
Proactively, not just reactively. Have a clear purpose for the engagement - an insight you want to gather, a piece of education you want to deliver. Open the email with what you're working on, not who you are. Be specific about what you'd like from them and what you'll bring in return. Keep the first contact short. The goal is a conversation, not a presentation.
"Why would an HCP value my input when I work in Pharma or I’m not a clinician?"
Because you bring something they don't have: cross-institutional synthesis. They see their patients. You see patterns across the wider evidence base, across multiple sites, across the pipeline. Your value isn't clinical experience - it's perspective. You're the expert on your data. If you're gathering insights, close the loop - reach back to the HCP and tell them how their input shaped your strategy. It's not a one-way data dump; it's a relationship. The earlier you internalise this, the easier the conversations become.
"What do I say in a first email to a KOL?"
Short. Specific. Scientific. Introduce yourself in one line. Name the reason for the contact - an introduction, a request to meet to discuss insights, a clinical question, an upcoming meeting. Ask for what you want clearly - that’s where the value add is.
"How do I build a KOL plan when I haven't been given a clear objective?"
Go back to your manager. A KOL plan without an objective isn't a KOL plan - it's a list. Push for the underlying question: are you trying to build advocacy for an upcoming launch, gather insight on a specific clinical question, develop investigators for a study? Each leads to a different plan. If your manager genuinely doesn't know, that's information too - and the conversation that follows is more useful than building the wrong plan in silence.
"What's the difference between promotional and non-promotional activity?"
Promotional = intended to encourage prescribing, restricted to on-licence information, owned by Commercial.
Non-promotional = legitimate scientific exchange, can include reactive off-licence discussion, owned by Medical Affairs. The line is about intent and framing, not just topic. The same data can be discussed in either context depending on how and why. See the dedicated section above.
"How do I demonstrate the value I'm bringing?"
By tying activities to outcomes, not activity counts. Insights generated and how they've shaped strategy. Education delivered and what shifted as a result. KOL relationships built and what's now possible because of them. The shift is from "what did I do this quarter" to "what changed because of what I did." Genuinely hard at first; it gets easier with practice and a framework.
"Who should I be working with internally?"
Brand team (Marketing, Commercial, Market Access, Regulatory, Medical), R&D and clinical development (especially pre-launch and during late-phase studies), Patient Advocacy, Public Affairs, Compliance, and your wider regional or global Medical organisation. The map varies by company. Ask for an org chart, and ask who attends the brand team meetings - that's a fast way to understand the actual structure.
"How do I present clinical data without sounding like a clinical paper?"
Lead with the question the data answers, not the methodology. Don’t drown them with the data! Structure as a story: what was known, what was unknown, what we found, what it means. Strip out non-essential statistics. Use one well-designed chart instead of three crowded ones. Rehearse out loud - clinical narrative is a spoken skill before it's a written one.
"How do I prepare for an advisory board?"
Start with the objective - what do you actually need to learn that you don't already know? Design the question flow backwards from there. Brief the chair so they understand the discussion you're trying to enable. Select participants based on the question, not seniority alone. After the meeting, synthesise the insights into a report the business can actually use - this is where most advisory boards lose their value.
Why even experienced hires often have these gaps
A pattern I see across the industry: companies hire "experienced" Medical Affairs people on the assumption that they arrived with the foundations in place.
Often, they didn't.
They learned the way everyone else did - by osmosis, by mistakes, by occasionally catching a senior colleague at a quiet moment. They have deep knowledge of their previous therapy area. They have specific operational experience. But the underlying foundations - the role of Medical across the lifecycle, the principles of strategic activity selection, what to do when, the frameworks for cross-functional alignment - may never have been formally taught.
It's not a person problem. It's a system problem. The industry undertrains the function as a whole and then assumes lateral hires bring with them what their previous employer also failed to teach.
The implication: structured foundational learning isn't only for the newest hires. It's often a useful reset for people several years into the role who quietly know they have gaps and have never had a clean way to fill them.
The real cost of leaving people to figure it out
When new hires are left without structured onboarding, four things happen consistently.
Loss of confidence. Capable people start to doubt themselves. They hesitate before sending emails. They second-guess in cross-functional meetings. The imposter narrative compounds.
Slow decision-making. Without frameworks, every decision is a first-principles decision. People escalate unnecessarily. They wait for permission they don't need. The function looks less senior than it is.
Cross-functional friction. When Medical Affairs can't clearly articulate what it owns, Marketing fills the vacuum. Commercial fills the vacuum. The Medical voice gets quieter in brand team meetings - not because there's nothing to say, but because the new hire isn't sure what's safe to say yet.
Difficulty demonstrating impact. Six months in, the new hire has been busy. But asked to summarise what they've contributed, they struggle. That's a performance review problem. It's a bigger problem when budgets tighten and the function has to justify its headcount.
McKinsey explicitly names capability gaps as one of the four reasons Medical Affairs transformation has been slower than the 2030 vision requires. The gap isn't a personal failing. It's a structural one. But it gets paid for personally - by new hires, by their managers, and ultimately by the patients the function exists to serve.
What good support actually looks like
If you're a Medical Affairs leader, the fixable bit is here. You don't need a complete overhaul.
You need three things:
1. A structured grounding in the foundations. Not product training. Not compliance modules. The foundations - what Medical Affairs does across the lifecycle, what differentiates promotional from non-promotional activity, how to think about KOL engagement, how to interpret and present data, how to select activities that drive impact.
2. Practical resources and frameworks. Checklists for advisory boards. Templates for KOL outreach. Frameworks for thinking about the patient journey. New hires don't need theory - they need scaffolding they can hang their day-to-day work on.
3. A space to ask the questions they don't want to ask out loud. A peer community. A senior practitioner they can ask without looking unprepared with their manager. Somewhere "what do I say in this first email" gets answered by someone who's sent a thousand of them.
That's the essential framework for onboarding. The how matters less than getting the right building blocks in place.
Medical Affairs Essentials: the structured response
Medical Affairs Essentials is the course built specifically for this gap.
It's a CPD-accredited, self-paced foundational course for people in their first one to two years in Medical Affairs - Medical Advisors, MSLs, Medical Managers, and professionals transitioning into the function from clinical or scientific roles.
It covers:
→ The role of Medical Affairs across the product lifecycle - pre-launch, launch, post-launch
→ The promotional vs non-promotional distinction, with practical examples
→ How to engage with KOLs and external stakeholders
→ Critical data appraisal and how to present clinical evidence engagingly
→ How to run an effective advisory board
→ How to select the right Medical Affairs activity to drive impact at each stage
→ Digital engagement in a Medical Affairs context
Eight modules. Bite-sized. Self-paced. Twelve months of access to the modules, the practical resources (checklists, templates, glossaries), and the community - where I personally answer questions.
It's the structured version of what most of us got in fragments, on a good day, or over years, when a generous senior colleague had time.
You can view the full course brochure here, or email us directly to discuss enrolling a team.

Medical Affairs Essentials course
The bottom line
Medical Affairs is one of the most rewarding roles in pharma. It sits at the intersection of science, strategy, and human relationships. Done well, it shapes how patients are treated.
McKinsey's 2030 vision makes the strategic case clear: the function is becoming a coequal pillar of the pharmaceutical company alongside R&D and Commercial. The investment in capability has to catch up with the vision.
The route in is unnecessarily hard, and the industry's tolerance for that is wearing thin.
The hires you're losing in their first eighteen months aren't losing because they weren't capable. They're losing because they were dropped in without a map.
You can keep doing it the old way. Most companies still will.
Or you can be the one who closes the gap.
For Medical Affairs leaders
Get in touch about enrolling your team. We can discuss group enrolment, timing, and how the course fits alongside your existing onboarding.
For people early in their Medical Affairs career
The course is here. The investment is €799.50 and includes twelve months of access to modules, resources, and community.
If you want to make the case to your manager for this to be funded as part of your development plan, you can copy and adapt this:
"I'd like to invest in structured foundational training for Medical Affairs through the Medical Affairs Essentials course (CPD-accredited, €799.50). It covers the role across the lifecycle, the non-promotional framework, KOL engagement, and data presentation. It would shortcut several months of figuring things out and give me a stronger foundation for [specific upcoming work]. Can we discuss including it in this year's development budget?"
References
Algazy J, Garcia A, Ryan S, Westra A, Zemp A. A vision for medical affairs 2030: five priorities for patient impact. McKinsey & Company; October 2023.https://www.mckinsey.com/industries/life-sciences/our-insights/a-vision-for-medical-affairs-2030-five-priorities-for-patient-impact